Clinical patterns of Uveitis in a Regional Eye Institute of North India
Abstract
Background: Uveitis encompasses many conditions, all characterized by inflammation of the uveal tract either directly or indirectly. It can occur at any age but predominantly affects patients in the working-age group.
Objective: To report the clinical pattern of Uveitis in North India.
Settings and Design: A prospective study in a regional eye institute.
Methods: After taking informed consent, 100 patients with Uveitis aged 20–60 years were recruited from eye OPD between 2012- 2014. Detailed history, complete ophthalmic examination, standard diagnostic laboratory tests and radiographic studies wherever required were made.
Statistical analysis used: Descriptive.
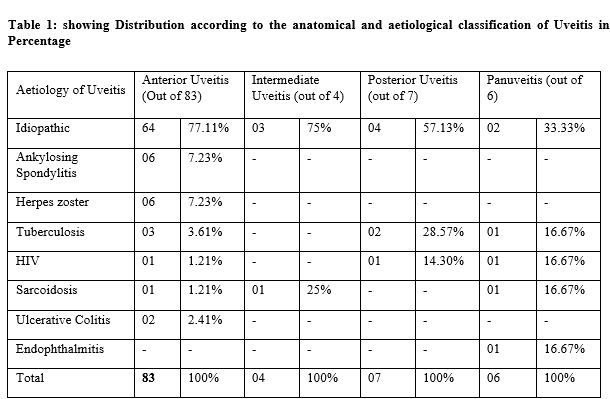
Results: The mean age being 41.55 years. There were 57% males and 43% females with 32% acute uveitis and 68% chronic uveitis cases. Anterior Uveitis was seen in 83% of patients, followed by posterior Uveitis (7%), pan-uveitis (6%) and intermediate Uveitis (4%). A definite association with the systemic disease was determined in 27% of cases. The most frequently observed systemic diseases were ankylosing spondylitis, Tuberculosis and herpes zoster ophthalmicus (6% cases each). This was followed by HIV (3%), sarcoidosis (3%), ulcerative colitis (2%) and endophthalmitis (1%). No specific aetiology or association with systemic diseases could be established in 73% of cases. In most cases, the systemic disease was not suspected before eye involvement and was recognized only after the subsequent diagnostic procedures.
Conclusion: The etiological diagnosis of Uveitis is often challenging as there are marked variations in ocular and systemic signs and symptoms. A significant number of cases may unfold with the evolution of advanced techniques.
Downloads
References
Nussenblatt RB. The natural history of Uveitis. Int Ophthalmol. 1990 Oct;14(5-6):303-8. doi: 10.1007/BF00163549.
Suttorp-Schulten MS, Rothova A. The possible impact of Uveitis in blindness: a literature survey. Br J Ophthalmol. 1996 Sep;80(9):844-8. doi: 10.1136/bjo.80.9.844.
Darrell RW, Wagener HP, Kurland LT. Epidemiology of Uveitis. Incidence and prevalence in a small urban community. Arch Ophthalmol. 1962 Oct;68:502-14. doi: 10.1001/archopht.1962.00960030506014.
Vadot, E., E. Barth, and P. Billet. Epidemiology of uveitis-preliminary-results of a prospective-study in savoy. acta ophthalmologica. Dept ohpthalmology, dk-8000 aarhus, denmark: arhus univ hospital, 1984.
Baarsma GS. The epidemiology and genetics of endogenous Uveitis: a review. Curr Eye Res. 1992;11 Suppl:1-9. doi: 10.3109/02713689208999505.
Tran VT, Auer C, Guex-Crosier Y, Pittet N, Herbort CP. Epidemiology of Uveitis in Switzerland. Ocul Immunol Inflamm. 1994;2(3):169-76. doi: 10.3109/09273949409057073.
Dandona L, Dandona R, John RK, McCarty CA, Rao GN. Population based assessment of Uveitis in an urban population in southern India. Br J Ophthalmol. 2000 Jul;84(7):706-9. doi: 10.1136/bjo.84.7.706.
Jabs DA, Nussenblatt RB, Rosenbaum JT; Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005 Sep;140(3):509-16. doi: 10.1016/j.ajo.2005.03.057.
Weiner A, BenEzra D. Clinical patterns and associated conditions in chronic Uveitis. Am J Ophthalmol. 1991 Aug 15;112(2):151-8. doi: 10.1016/s0002-9394(14)76694-2.
Nakahara H, Kaburaki T, Takamoto M, Okinaga K, Matsuda J, Konno Y, et al. Statistical analyses of Endogenous Uveitis Patients (2007-2009) in central Tokyo area and Comparison with Previous Studies (1963-2006). Ocul Immunol Inflamm. 2015 Aug;23(4):291-296. doi: 10.3109/09273948.2014.920036.
Goto H, Mochizuki M, Yamaki K, Kotake S, Usui M, Ohno S. Epidemiological survey of intraocular inflammation in Japan. Jpn J Ophthalmol. 2007 Jan-Feb;51(1):41-4. doi: 10.1007/s10384-006-0383-4.
Keino H, Nakashima C, Watanabe T, Taki W, Hayakawa R, Sugitani A, Okada AA. Frequency and clinical features of intraocular inflammation in Tokyo. Clin Exp Ophthalmol. 2009 Aug;37(6):595-601. doi: 10.1111/j.1442-9071.2009.02102.x.
Nakahara H, Kaburaki T, Tanaka R, Takamoto M, Ohtomo K, Karakawa A, et al. Frequency of Uveitis in the Central Tokyo Area (2010-2012). Ocul Immunol Inflamm. 2017;25(sup1):S8-S14. doi: 10.3109/09273948.2015.1133840.
Miettinen R. Incidence of Uveitis in Northern Finland. Acta Ophthalmol (Copenh). 1977 Apr;55(2):252-60. doi: 10.1111/j.1755-3768.1977.tb 01306.x.
Deschenes J, Murray PI, Rao NA, Nussenblatt RB; International Uveitis Study Group. International Uveitis Study Group (IUSG): clinical classification of Uveitis. Ocul Immunol Inflamm. 2008 Jan-Feb;16(1):1-2. doi: 10.1080/09273940801899822.
London NJ, Rathinam SR, Cunningham ET Jr. The epidemiology of Uveitis in developing countries. Int Ophthalmol Clin. 2010 Spring;50(2):1-17. doi: 10.1097/IIO.0b013e3181d2cc6b.
Rathinam SR, Namperumalsamy P. Global variation and pattern changes in the epidemiology of Uveitis. Indian J Ophthalmol. 2007 May-Jun;55(3):173-83. doi: 10.4103/0301-4738.31936.
Shams, Hormoz, et al. Epidemiology and prevalence of Uveitis: a literature review. 2009: 4-16.
Mercanti A, Parolini B, Bonora A, Lequaglie Q, Tomazzoli L. Epidemiology of endogenous uveitis in north-eastern Italy. Analysis of 655 new cases. Acta Ophthalmol Scand. 2001 Feb;79(1):64-8. doi: 10.1034/j.1600-0420.2001.079001064.x.
Khairallah M, Yahia SB, Ladjimi A, Messaoud R, Zaouali S, Attia S, et al. Pattern of uveitis in a referral centre in Tunisia, North Africa. Eye (Lond). 2007 Jan;21(1):33-9. doi: 10.1038/sj.eye.6702111.
Singh R, Gupta V, Gupta A. Pattern of Uveitis in a referral eye clinic in north India. Indian J Ophthalmol. 2004 Jun;52(2):121-5.
Das D, Bhattacharjee H, Bhattacharyya PK, Jain L, Panicker MJ, Das K, et al. Pattern of Uveitis in North East India: a tertiary eye care center study. Indian J Ophthalmol. 2009 Mar-Apr;57(2):144-6. doi: 10.4103/0301-4738.45506.
Shirahama S, Kaburaki T, Nakahara H, Tanaka R, Takamoto M, Fujino Y, et al. Epidemiology of Uveitis (2013-2015) and changes in the patterns of Uveitis (2004-2015) in the central Tokyo area: a retrospective study. BMC Ophthalmol. 2018 Aug 2;18(1):189. doi: 10.1186/s12886-018-0871-6.
Zheng Y, Zhang LX, Meng QL, Zhang M, Cui Y, Liu QY, et al. Clinical patterns and characteristics of Uveitis in a secondary hospital in southern China. Int J Ophthalmol. 2015 Apr 18;8(2):337-41. doi: 10.3980/j.issn.2222-3959.2015.02.22.
Biswas J, Narain S, Das D, Ganesh SK. Pattern of Uveitis in a referral uveitis clinic in India. Int Ophthalmol. 1996-1997;20(4):223-8. doi: 10.1007/BF00175264.
Jones NP. The Manchester Uveitis Clinic: the first 3000 patients--epidemiology and casemix. Ocul Immunol Inflamm. 2015 Apr;23(2):118-26. doi: 10.3109/09273948.2013.855799.
Copyright (c) 2021 Author (s). Published by Siddharth Health Research and Social Welfare Society

This work is licensed under a Creative Commons Attribution 4.0 International License.

 OAI - Open Archives Initiative
OAI - Open Archives Initiative





