Increased Incidence of Rhino-Orbital Mucormycosis in an Educational Therapeutic Hospital During The Covid-19 Pandemic: An Observational Study
Jethwa V.1, Vaghasia A.2, Sabnis M.3*
DOI: https://doi.org/10.17511/jooo.2023.i02.01
1 Vaidehi Jethwa, Junior resident, Department of Ophthalmology, Dr D.Y. Patil Medical College Hospital and Research Institute, Kolhapur, Maharashtra, India.
2 Astha Vaghasia, Junior resident, Department of Ophthalmology, Dr D.Y. Patil Medical College Hospital and Research Institute, Kolhapur, Maharashtra, India.
3* Milind Sabnis, Professor and HOD, Department of Ophthalmology, Dr D.Y. Patil Medical College Hospital and Research Institute, Kolhapur, Maharashtra, India.
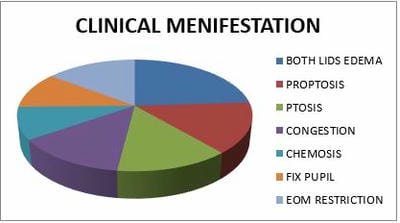
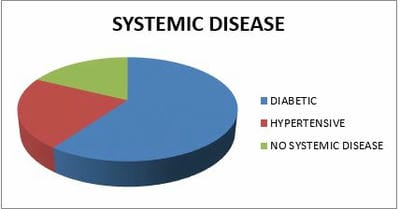
Introduction: Coronavirus had become an emergency in 2019. At that time invasive mucormycosis post-COVID-19 also emerged. There are multiple case reports and series describing mucormycosis in COVID-19. The recent emergence of the Coronavirus Disease (COVID-19) disease had been associated with reports of fungal infections such as aspergillosis and mucormycosis especially among critically ill patients like immune-compromised patients who have been treated with steroids. Method: A cross-sectional was conducted on patients with MRI and biopsy-proven mucormycosis with RT-PCR-confirmed COVID-19 from May to August 2021 at Dr D. Y. Patil Medical College and Research Institute, kadamwadi, Kolhapur, Maharashtra, India. the time interval between COVID-19 and mucormycosis, underlying systemic diseases, clinical features, course of the disease, and outcomes were collected and analyzed. (n=32). Result: out of 45 mucormycosis patients, 10 were female and 35 were male. The youngest participant was aged 12 years, and the oldest was 75 years old, the mean age was 53.33 ± 14.99 years. The majority of patients, 27 (60%) are diabetic and 10 are hypertensive (22.22%). 28 patients were COVID-19 positive. And 66.67% of patients were rhino orbital type of mucormycosis. All patients were treated with Amphotericin-B but out of 11(24.44%) got transcutaneous retrobulbar amphotericin –B injection. Conclusion: SARS-COV-2 infected patient numbers were increasing in COVOD -19 pandemic. Mucormycosis proved itself an epidemiological burden. So risk-based approach for patients with risk is necessary. Attention was to be given to that patients who were diabetic (uncontrolled sugar level), on combined use of steroids, or immune-modulating agents.
Keywords: Coronavirus, Rhino-Orbital mucormycosis, Aspergillosis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Professor and HOD, Department of Ophthalmology, Dr D.Y. Patil Medical College Hospital and Research Institute, Kolhapur, Maharashtra, India. Email:  |
Vaidehi Jethwa, Astha Vaghasia, Milind Sabnis, Increased Incidence of Rhino-Orbital Mucormycosis in an Educational Therapeutic Hospital During The Covid-19 Pandemic: An Observational Study. Trop J Ophthalmol Otolaryngol. 2023;8(2):6-10. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/246 |
 |
 ©
©  Figure 1: Histopathologically positive slide of mucormycosis given after debridement surgery.
Figure 1: Histopathologically positive slide of mucormycosis given after debridement surgery. Figure 2: MRI showing mucormycosis in maxillary sinus and orbit.
Figure 2: MRI showing mucormycosis in maxillary sinus and orbit.