A late presented case of a pseudophakic bullous keratopathy with Descemet's membrane detachment treated by penetrating keratoplasty
Prasad N.1*, Dubey A.2, Kumar K.3
DOI: https://doi.org/10.17511/jooo.2022.i06.03
1* Nishi Prasad, Junior Resident, Third Year, Department of Ophthalmology, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
2 Aditi Dubey, Associate Professor, Department of Ophthalmology, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
3 Kavita Kumar, Professor & Head, Department of Ophthalmology, Gandhi Medical College, Bhopal, Madhya Pradesh, India.
Pseudophakic bullous keratopathy (PBK), also known as postoperative corneal edema, is the development of irreversible corneal edema after cataract surgery. Descemet’s membrane detachment (DMD) is also relatively common after cataract surgery. The purpose of this study is to present a case report on the visual outcome after penetrating keratoplasty in an elderly female with longstanding pseudophakic bullous keratopathy with descemet’s membrane detachment, who presented to cornea clinic with gradual progressive diminution of vision, five years after cataract surgery. Penetrating keratoplasty with a healthy donor cornea helped salvage her visual outcome.
Keywords: Pseudophakic bullous keratopathy, Descemet’s membrane detachment, Penetrating keratoplasty, Visual outcome
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Junior Resident, Third Year, Department of Ophthalmology, Gandhi Medical College, Bhopal, Madhya Pradesh, India. Email:  |
Nishi Prasad, Aditi Dubey, Kavita Kumar, A late presented case of a pseudophakic bullous keratopathy with Descemet's membrane detachment treated by penetrating keratoplasty. Trop J Ophthalmol Otolaryngol. 2022;7(6):46-49. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/243 |
 |
 ©
©  Fig 1: left eye cornea showing pseudophakic bullous keratopathy
Fig 1: left eye cornea showing pseudophakic bullous keratopathy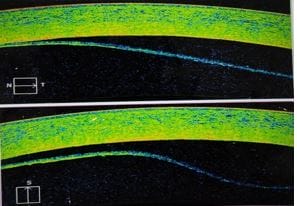 Fig 2: Left eye anterior segment OCT showing Descemet's membrane detachment
Fig 2: Left eye anterior segment OCT showing Descemet's membrane detachment Fig 3: Post-penetrating keratoplasty after 1 week with healthy graft
Fig 3: Post-penetrating keratoplasty after 1 week with healthy graft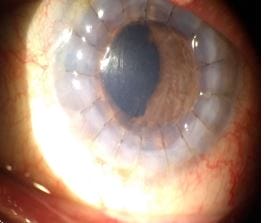 Fig 4: Post-penetrating keratoplasty after 2 weeks with healthy graft
Fig 4: Post-penetrating keratoplasty after 2 weeks with healthy graft