Can Myopia Be Reversed? - A Study on the Role of Atropine Eye drops in Arresting Myopia Progression
Tripathi A.1*, Gupta R.2, Mohan S.3
DOI: https://doi.org/10.17511/jooo.2021.i06.02
1* Anchal Tripathi, Senior Resident, Department of Ophthalmology, GSVM Medical College, Kanpur, U.P, India.
2 RC Gupta, Professor and Head, Department of Ophthalmology, LLRM, Meerut, U.P, India.
3 Shalini Mohan, Associate Professor, Department of Ophthalmology, GSVM Medical college, Kanpur, U.P, India.
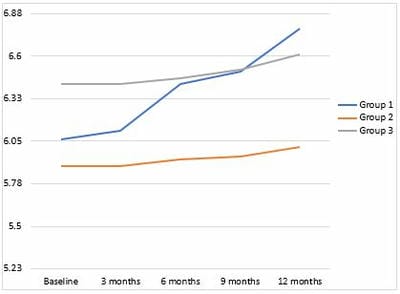
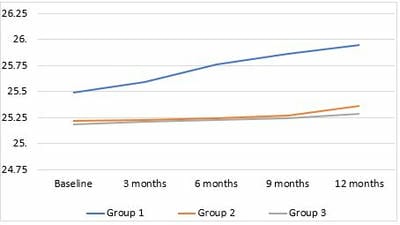
Introduction: Atropine is being explored as a potent agent for arresting myopia progression for ages. In our study, we attempt to investigate the efficacy of two different concentrations of atropine in halting myopia progression in Indian eyes. Objectives: 1. To investigate the effect of atropine in retarding progression of myopia. 2. To compare rates of retardation of myopia progression using 0.05% atropine and 0.1% atropine. Methods: Patients were selected from children between 6-18 yrs of age, visiting the outpatient department of our hospital, with spherical equivalent (SE) =>-1D in both the eyes and spherical equivalent (SE) progression rate >= 0.5D/year. Groups with 0.05% atropine eye drop, 0.1% atropine eye drops and control were allocated randomly. Myopia progression was measured by the change in spherical equivalent and axial length at baseline and every three months till one year. Results: In our study, a total of 48 eyes of 24 children were included, out of which 83.33% were in the age group 6-12years. The mean change in spherical equivalent in our study after one year was -0.72±0.21D, -0.11±0.096D and -0.19±0.18D in control, 0.1% and 0.05% atropine groups, respectively. Also, the mean change in axial length of our study after one year was 0.45±0.15mm, 0.13±0.20mm and 0.11±0.02mm in control, 0.1% and 0.05% atropine groups, respectively. Changes in both parameters were found to be statistically significant. Conclusion: We conclude that night-time application of 0.05% and 0.1% atropine eye drops is efficacious in retarding progressive myopia in Indian eyes.
Keywords: Atropine, Axial length, Myopia, Spherical equivalent
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior Resident, Department of Ophthalmology, GSVM Medical College, Kanpur, U.P, India. Email:  |
Anchal Tripathi, RC Gupta, Shalini Mohan, Can Myopia Be Reversed? - A Study on the Role of Atropine Eye drops in Arresting Myopia Progression. Trop J Ophthalmol Otolaryngol. 2021;6(6):114-120. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/217 |
 |
 ©
©