The Outcome of Intratympanic Dexamethasone Treatment on Idiopathic Sudden Sensorineural Hearing Loss
Yamuna R.1, Archana U.2*, Shaiju A.3, Mohan C.4
DOI: https://doi.org/10.17511/jooo.2022.i01.03
1 R Yamuna, Assistant Professor, ENT, GMC, Thiruvananthapuram, Kerala, India.
2* U M Archana, Assistant Surgeon, PHC, PHC, Kannambra, Palakkad, Kerala, India.
3 A Shaiju, Assistant Professor, ENT, GMC, Thiruvananthapuram, Kerala, India.
4 Chippy Mohan, Assistant Professor, Audiology, GMC, Thiruvananthapuram, Kerala, India.
Introduction: Sudden sensorineural hearing loss is a frustrating symptom which when detected early can be treated with oral, intra venous or intra tympanic steroids. Objective: To assess the effectiveness of intra tympanic steroid injection in idiopathic sensorineural hearing loss. Method: A follow-up study done was among patients satisfying the case definition of idiopathic sudden sensorineural hearing loss. 35 Patients were evaluated by taking clinical history and performing complete physical examination. Pure tone audiogram was performed before and after intratympanic dexamethasone injection and recovery was analyzed. Result: After statistical analysis overall outcome of the hearing was found better with intratympanic dexamethasone injection therapy. Conclusion: Intratympanic dexamethasone therapy was useful in patients with idiopathic sudden sensorineural hearing loss.
Keywords: Idiopathic sudden sensorineural hearing loss, Intratympanic dexamethasone injection
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Surgeon, PHC, PHC, Kannambra, Palakkad, Kerala, India. Email:  |
R Yamuna, U M Archana, A Shaiju, Chippy Mohan, The Outcome of Intratympanic Dexamethasone Treatment on Idiopathic Sudden Sensorineural Hearing Loss. Trop J Ophthalmol Otolaryngol. 2022;7(1):12-17. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/211 |
 |
 ©
© 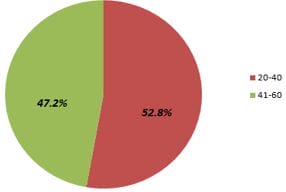 Figure 1: Age distribution of patients.
Figure 1: Age distribution of patients.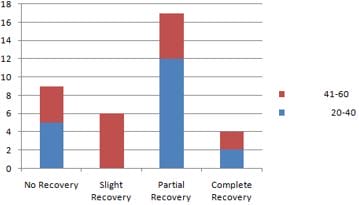 Figure 2: Recovery of patients who received intratympanic dexamethasone treatment according to age group.
Figure 2: Recovery of patients who received intratympanic dexamethasone treatment according to age group.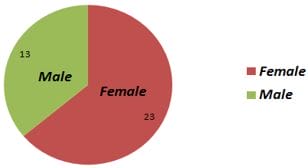 Figure 3: Sex distribution of patients.
Figure 3: Sex distribution of patients.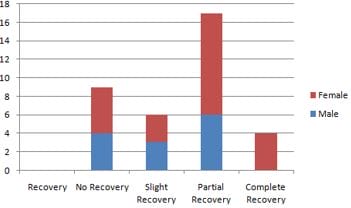 Figure 4: Recovery Rate among males and females.
Figure 4: Recovery Rate among males and females.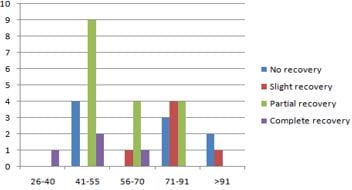 Figure 5: Recovery according to pretreatment Hearing loss.
Figure 5: Recovery according to pretreatment Hearing loss.