A retrospective study to analyse the ocular morbidity in the slum-dwelling population of central India
Shrivastava P.1*, soni A.2, kumar S.3, shrivastava L.4
DOI: DOI: https://doi.org/10.17511/jooo.2021.i04.03
1* Poorva Shrivastava, Senior resident, , Gandhi medical college, Bhopal, Madhya Pradesh, India.
2 Apoorva soni, Senior resident, , Gandhi medical college, Bhopal, Madhya Pradesh, India.
3 Salil kumar, Ex-consultant, ophthalmologist, Gandhi medical college, Bhopal, Madhya Pradesh, India.
4 Lalit shrivastava, Consultant, ophthalmologist, Kamla Nehru Hospital, Bhopal, Madhya Pradesh, India.
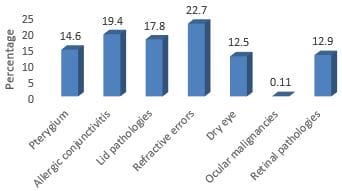
Background: The study aimed to evaluate the prevalence of different ocular pathologies in the slum-dwelling population of central India and to find its correlations with socio-demographic factors. Methodology: The study was conducted as a cross-sectional study in 84 slum areas across Bhopal, Jabalpur and areas in the vicinity using a camp-based approach during the study period of 3 years. A total of 15478 participants attended the camp, and of them, 6177 patients had various ophthalmological conditions. A detailed history was obtained, and participants were subjected to a complete ophthalmological examination. Based upon their diagnosis, they were prescribed treatment. Referral to the tertiary care centre was done when needed. Results: The prevalence of ocular morbidities was 39.9%. The most common ocular morbidity documented in our study was refractive errors (22.7%). Proportions of lid pathologies were significantly higher in patients belonging to less than ten years of age (36.4%). In contrast, refractive errors were observed in higher proportions of patients belonging to more than ten years of age (p<0.05). Pterygium ratio was significantly higher in males, whereas ocular malignancies were higher in females (p<0.05). Proportions of almost all the ocular morbidities were substantially higher in patients with low socioeconomic status (p<0.05). Conclusion: The overall prevalence of ocular morbidities in the slum population is high. The most common ocular morbidity includes refractive error and allergic conjunctivitis. These morbidities correlated with age, gender and socioeconomic status. We recommend periodic screening of the slum population across all age range to prevent long term complications and disabilities.
Keywords: Ocular morbidity, Slum, Refractive errors, Age, Socioeconomic status
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Senior resident, , Gandhi medical college, Bhopal, Madhya Pradesh, India. Email:  |
Poorva Shrivastava, Apoorva soni, Salil kumar, Lalit shrivastava, A retrospective study to analyse the ocular morbidity in the slum-dwelling population of central India. Trop J Ophthalmol Otolaryngol. 6;4(2021):69-74. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/202 |
 |
 ©
©