A study of the correlation between smartphone usage and dry eye in medical students at a tertiary care center
Faruqui S.1, Agarwal R.2, Kumar R.3*
DOI: https://doi.org/10.17511/jooo.2020.i07.02
1 Saba Faruqui, Assistant Professor, Department of ophthalmology, LN Medical College and JK Hospital, Bhopal, Madhya Pradesh, India.
2 Rahul Agarwal, Professor and Head, Department of ophthalmology, LN Medical College and JK Hospital, Bhopal, Madhya Pradesh, India.
3* Rashmi Kumar, Associate Professor, Department of ophthalmology, LN Medical College and JK Hospital, Bhopal, Madhya Pradesh, India.
Background: CVS and dry eye disease due to computers, in general, is well documented, but specific literature on smartphone usage leading to these conditions is limited. This study aims to estimate the prevalence of dry eye and determine the effect of duration of use on the CVS symptoms in college-going smartphone users. Aims: (1) To find a correlation between smartphone usage and dry eye(2)To find the prevalence of dry eye disease in the smartphone using college students (3)To study whether the duration and pattern of smartphone usage has a bearing on the severity of CVS symptoms. Materials and Methods: 394 medical students using smartphones for over a year and without pre-existing dry eye disease or ocular surface pathology were included. Tear film parameters were estimated. The duration of use and smartphone settings were correlated with the prevalence of dry eye and computer vision syndrome symptoms. Results: The prevalence of dry eye was 20.81%. The average DED score was 1.56±0.234, and 1.35±0.248 respectively in the DED and non-DED group with a p-value of 0.0001. The most common CVS symptoms were fatigue (54% in DED,44% in non-DED) and heaviness in both groups (60.9% in DED, 45% in non-DED group.). Conclusions: There was a statistically significant increase in the DED symptom score and the prevalence of CVS symptoms with increasing duration of use and daily exposure to smartphones.
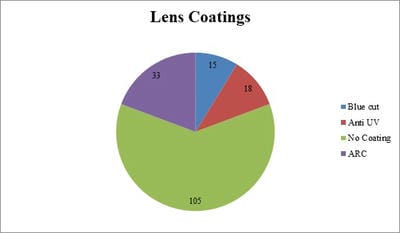
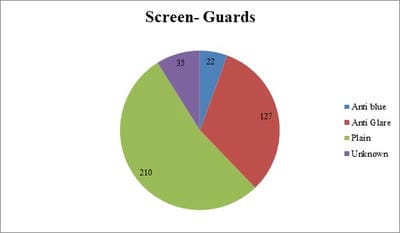
Keywords: Smartphone, Dry eye disease, Computer vision syndrome, Blue filters, Screen guard
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of ophthalmology, LN Medical College and JK Hospital, Bhopal, Madhya Pradesh, India. Email:  |
Faruqui S, Agarwal R, Kumar R. A study of the correlation between smartphone usage and dry eye in medical students at a tertiary care center. Trop J Ophthalmol Otolaryngol. 2020;5(7):174-182. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/165 |
 |
 ©
©