A Rare Case of Congenital Eyelid Imbrication Syndrome and Floppy Eyelid Syndrome
Ambre A.1*, M Sabnis M.2, Linga Sai Greeshma Reddy B.3
DOI: https://doi.org/10.17511/jooo.2022.i06.01
1* Aishwarya Ambre, Resident, Department of ophthalmology, Dr D. Y. Patil medical college, hospital and research institute, Kolhapur, Maharashtra, India.
2 Milind M Sabnis, Professor and HOD, Department of ophthalmology, Dr D. Y. Patil medical college, hospital and research institute, Kolhapur, Maharashtra, India.
3 Bobbiti Linga Sai Greeshma Reddy, Resident, Department of ophthalmology, Dr D. Y. Patil medical college, hospital and research institute, Kolhapur, Maharashtra, India.
Congenital eyelid imbrication syndrome (CEIS) is an exceptionally rare, benign, short-lasting, self-limiting eyelid malposition disorder. The classical triad consists of bilateral upper eyelids overriding the lower eyelids, bilateral medial and lateral canthal tendon laxity, and tarsal conjunctival congestion. We report a case of congenital combined eyelid imbrication and floppy eyelid syndrome in a healthy neonate that was resolved within five days with conservative management. In adults, eyelid imbrication is usually associated with floppy eyelid syndrome which requires surgical correction.
Keywords: Floppy Eyelids, Eyelid Imbrication, Tendon Laxity, Eyelid Malposition, CEIS
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Resident, Department of ophthalmology, Dr D. Y. Patil medical college, hospital and research institute, Kolhapur, Maharashtra, India. Email:  |
Aishwarya Ambre, Milind M Sabnis, Bobbiti Linga Sai Greeshma Reddy, A Rare Case of Congenital Eyelid Imbrication Syndrome and Floppy Eyelid Syndrome. Trop J Ophthalmol Otolaryngol. 2022;7(6):39-41. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/241 |
 |
 ©
©  Fig 1: Clinical photograph of the neonate with congenital
Fig 1: Clinical photograph of the neonate with congenital Fig 2: Clinical photograph of the neonate with congenital eyelid imbrication and floppy eyelid syndrome showing eyelid imbrication and floppy eyelid syndrome overlapping of the upper lid over the lower lid showing spontaneous eversion of the upper lid on gentle pulling of the skin of the upper lid.
Fig 2: Clinical photograph of the neonate with congenital eyelid imbrication and floppy eyelid syndrome showing eyelid imbrication and floppy eyelid syndrome overlapping of the upper lid over the lower lid showing spontaneous eversion of the upper lid on gentle pulling of the skin of the upper lid.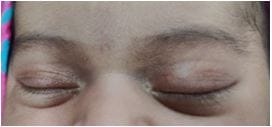 Figure 3: Clinical photograph of the neonate with congenital eyelid imbrication and floppy eyelid syndrome on day 5 showing the resolution.
Figure 3: Clinical photograph of the neonate with congenital eyelid imbrication and floppy eyelid syndrome on day 5 showing the resolution.