Multi-layered amniotic membrane transplantation for the management of corneal ulcers during the Covid pandemic
Joshi S.1*, Joshi H.2, Abhyankar A.3, Madan Deshpande C.4
DOI: https://doi.org/10.17511/jooo.2022.i05.01
1* Shilpa Joshi, Cornea Consultant & H.O.D, Medical Director Eye Bank, H.V. Desai Eye Hospital, Pune, Maharashtra, India.
2 Hema Joshi, Cornea Consultant, H.V. Desai Eye Hospital, Pune, Maharashtra, India.
3 Anannya Abhyankar, DNB Final year resident, H.V. Desai Eye Hospital, Pune, Maharashtra, India.
4 Col. Madan Deshpande, Chief Medical Director, H.V. Desai Eye Hospital, Pune, Maharashtra, India.
This study was done to assess the outcome of multilayer amniotic membrane transplantation (AMT) for severe progressive fungal keratitis & perforated corneal ulcers. With the COVID-19 pandemic-related lockdown and unavailability of donor corneas, multi-layered AMT was done in these cases. We hereby report nine such cases, all of which showed reduced inflammation, resolution of infiltrates, good epithelisation and no recurrence of infection. None needed TPK in subsequent weeks of follow-up. With palliative treatment of AMT, eyes with vision-threatening keratitis can be salvaged, till the availability of donor corneas.
Keywords: Multilayer amniotic membrane transplantation, COVID-19, Fungal keratitis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Cornea Consultant & H.O.D, Medical Director Eye Bank, H.V. Desai Eye Hospital, Pune, Maharashtra, India. Email:  |
Shilpa Joshi, Hema Joshi, Anannya Abhyankar, Col. Madan Deshpande, Multi-layered amniotic membrane transplantation for the management of corneal ulcers during the Covid pandemic. Trop J Ophthalmol Otolaryngol. 2022;7(5):32-38. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/233 |
 |
 ©
© 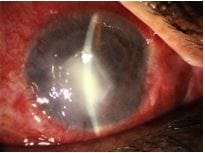

 Figure 1C: Post healing- adherent leucoma
Figure 1C: Post healing- adherent leucoma Figure 1D: Post-Optical Keratoplasty
Figure 1D: Post-Optical Keratoplasty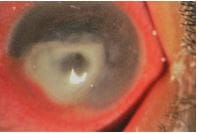 Figure 2A:Perforated fungal ulcer
Figure 2A:Perforated fungal ulcer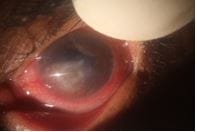 Figure 2B: Post multi-layered AMG
Figure 2B: Post multi-layered AMG

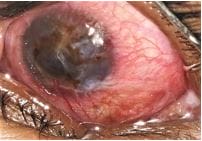
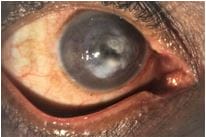 Figure 4A:Corneal ulcer with large descemetocele
Figure 4A:Corneal ulcer with large descemetocele Figure 4B:Post-AMG healed ulcer with anterior staphyloma
Figure 4B:Post-AMG healed ulcer with anterior staphyloma