Comparative Study of Clinical Outcome between Microscopic and Endoscopic Type I Tympanoplasty
Yadav M.1*, Hussain R.2, Monga J.3, Naik S.4
DOI: https://doi.org/10.17511/jooo.2021.i06.03
1* Mayank Yadav, Assistant Professor, Department of Otorhinolaryngology, SHKM GMC, Nuh, Haryana, India. ORCID: 0000-0002-9729-752X
2 Raj Tajamul Hussain, Senior Registrar, Department of Otorhinolaryngology, SHKM GMC, Nuh, Haryana, India. ORCID: 0000-0002-9795-3697
3 Jasdeep Monga, Associate professor, Department of Otorhinolaryngology, SHKM GMC, Nuh, Haryana, India. ORCID: 0000-0001-5764-063X
4 S.M. Naik, Professor, Department of Otorhinolaryngology, SHKM GMC, Nuh, Haryana, India. ORCID: 0000-0002-7159-5019
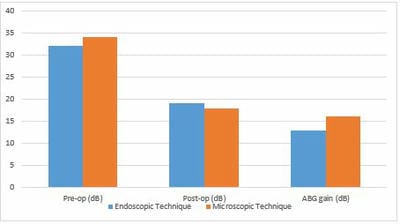
Introduction: Tympanoplasty is one of the most common surgical procedures in ENT. It can be performed with the help of a microscope or endoscope. We carried out a prospective randomized comparative study in our tertiary care centre to evaluate and compare the results of endoscopic and conventional microscopic tympanoplasty in terms of hearing outcome, surgical time and graft success rate. Materials and Methods: This prospective randomized comparative study was conducted in the Department of Otorhinolaryngology, SHKM Hospital, an associated hospital of GMC Nuh, Haryana, India, for 12 months from October 2019 to September 2020. Eighty patients with central perforation were randomly divided into two equal groups of 40 patients each. In the first group, an endoscope was used, and in the second group, the microscope was used to do type 1 tympanoplasty. The patients were kept on follow-up for six months. The graft success rates, hearing outcomes and duration of surgery in patients were compared in both groups. Results: Graft success rates were 90% and 92.5% for the endoscopic and microscopic groups, respectively (p > 0.05). Postoperative air-bone gap values significantly improved in both groups (p < 0.05). The average duration of surgery was significantly shorter in the endoscopic group (mean 42.9 min) relative to the microscopic group (mean 57.2 min) (p < 0.05). Conclusion: In managing chronic otitis media, endoscopic transcanal tympanoplasty can be a viable alternative to conventional microscopic tympanoplasty, with comparable graft success rates and hearing outcomes.
Keywords: CSOM. Endoscopic tympanoplasty. Microscopic tympanoplasty, Perforation, Operative duration, ABG
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Otorhinolaryngology, SHKM GMC, Nuh, Haryana, India. Email:  |
Mayank Yadav, Raj Tajamul Hussain, Jasdeep Monga, S.M. Naik, Comparative Study of Clinical Outcome between Microscopic and Endoscopic Type I Tympanoplasty. Trop J Ophthalmol Otolaryngol. 2021;6(6):121-127. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/226 |
 |
 ©
©