Bilateral Combined central retinal artery and vein occlusion (CCRAVO) in COVID-19 patient
Ganekal S.1*, Dorairaj S.2, Ganekal V.3
DOI: https://doi.org/10.17511/jooo.2021.i06.04
1* Sunil Ganekal, Research Collaborator, Department of Ophthalmology, Mayo Clinic College of Medicine, , Florida, USA.
2 Syril Dorairaj, Fellowship, Department of Ophthalmology, Mayo Clinic College of Medicine, , Florida, USA.
3 Varun Ganekal, Research Assistant, Department of Ophthalmology, , Davangere, Karnataka, India.
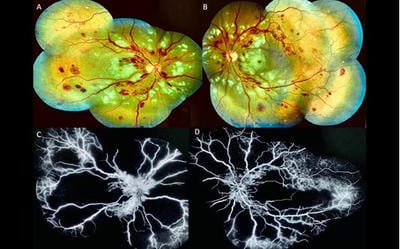
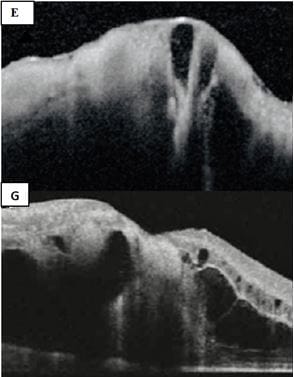
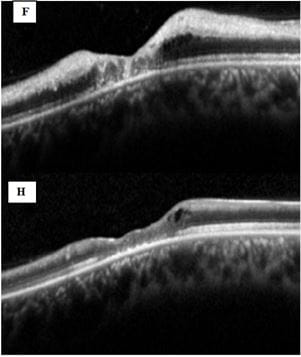
We report a case of a male patient who gave a history of fever, dry cough, dyspnea and he was tested positive for COVID-19 by Reverse Transcriptase-PCR from the nasopharynx. Presented with the sudden bilateral onset of decreased vision due to combined central retinal artery and vein occlusion (CCRAVO), the patient was treated with systemic medication including anticoagulant treatment and Intravitreal bevacizumab, and visual recovery was limited despite treatment.
Keywords: Combined central retinal artery and vein occlusion, COVID-19
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Research Collaborator, Department of Ophthalmology, Mayo Clinic College of Medicine, , Florida, USA. Email:  |
Sunil Ganekal, Syril Dorairaj, Varun Ganekal, Bilateral Combined central retinal artery and vein occlusion (CCRAVO) in COVID-19 patient. Trop J Ophthalmol Otolaryngol. 2021;06(06):128-131. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/222 |
 |
 ©
©