Clinical Profile of Proptosis in a Tertiary Eye Care Hospital in Central India
Sinha A.1*
DOI: https://doi.org/10.17511/jooo.2021.i06.01
1* Abha Sinha, Associate Professor, Department of Ophthalmology, BRLSABVM Medical College, Rajnandgaon, Chhattisgarh, India.
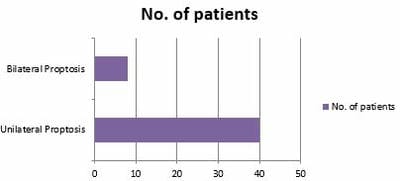
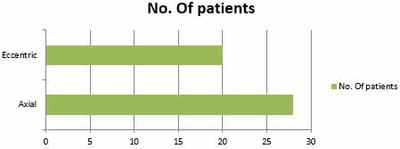
Introduction: Proptosis is the protrusion or forward displacement of one or both eyeballs from posterior pressure on the globe due to increased orbital volume either from intraorbital or intracranial space-occupying lesion. This study aims to find out the aetiology, clinical features, and its management. Material and Methods: Study setting- Department of ophthalmology, BRLSABVM Medical College, Rajnandgaon (C.G.), India. Study duration- July 2017 to June 2020. Type of study- Prospective study. Sampling methods- Universal sampling method. Sample size- 875 patients presenting with provisional diagnosis of proptosis over three years were included. Results: In the present study, 875 patients presented with a provisional diagnosis of proptosis; out of them in only 48 patients confirmed proptosis was seen. In the present study, it was found more common in males than females. The most common aetiology of proptosis in the present study was orbital cellulitis; among them, two had bilateral proptosis. The neoplasm was the second most common cause of proptosis, affecting 13 eyes of 11 patients. The most common symptoms were protrusion of the eye followed by eye pain & headache. Other symptoms were diminished vision, diplopia, diminished motility, epiphora, chemosis & proptosis. Conclusion: Present study showed that the most common cause of proptosis is orbital cellulitis. The etiology and pathogenesis of proptosis are diverse, which can be vision or life-threatening, highlighting the need for early and timely diagnosis of these cases, mandating various spectrum of investigations.
Keywords: Proptosis, Exophthalmometer, Orbital cellulitis
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Associate Professor, Department of Ophthalmology, BRLSABVM Medical College, Rajnandgaon, Chhattisgarh, India. Email:  |
Abha Sinha, Clinical Profile of Proptosis in a Tertiary Eye Care Hospital in Central India. Trop J Ophthalmol Otolaryngol. 2021;6(6):108-113. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/219 |
 |
 ©
©