Window technique for Hematoma Auris / Seroma – A Promising technique
Wahid S.1, Susmitha S.2*, Yedluri S.3, Dinesh A.4
DOI: https://doi.org/10.17511/jooo.2021.i05.03
1 Sk Wahid, Assistant Professor, Department of Otorhinolaryngology, NRI Academy of Sciences, Guntur, Andhra Pradesh, India.
2* Satujoda Susmitha, Post Graduate, Department of Otorhinolaryngology, NRI Academy of Sciences, Guntur, Andhra Pradesh, India.
3 Satya Prabhakar Rao Yedluri, Professor and HOD, Department of Otorhinolaryngology, NRI Academy of Sciences, Guntur, Andhra Pradesh, India.
4 Aradhyula Dinesh, Post Graduate, Department of Otorhinolaryngology, NRI Academy of Sciences, Guntur, Andhra Pradesh, India.
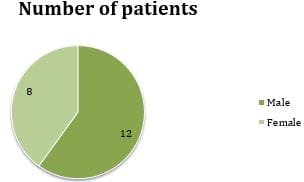
Background: The seroma of the pinna is the accumulation of serous fluid between the perichondrium and cartilage of the pinna. Despite several surgical techniques in the treatment of seroma, recurrence is common. The aim and objective of this preliminary study are to present and discuss a novel approach in treating pinna's pseudocyst. Materials and methods: A total of 20 patients with auricular seromas treated by window technique were included in the current study. Results: Results showed that all the patients tolerated the procedure well. No patient had any collection of fluid after the removal of the dressing. No patient experienced pain, fever, or oedema after the treatment. The seroma disappeared without disfigurement. There were no recurrences on further follow‑up. Conclusion: The window technique is a valuable technique for treating seroma and hematoma of pinna as the outcome is good with no recurrence.
Keywords: Hematoma Auris, Perichondrium, Seroma, Pinna, Cartilage, Serous fluid, Window technique, Pseudocyst
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Post Graduate, Department of Otorhinolaryngology, NRI Academy of Sciences, Guntur, Andhra Pradesh, India. Email:  |
Sk Wahid, Satujoda Susmitha, Satya Prabhakar Rao Yedluri, Aradhyula Dinesh, Window technique for Hematoma Auris / Seroma – A Promising technique. Trop J Ophthalmol Otolaryngol. 2021;6(5):99-104. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/201 |
 |
 ©
©