Comparison of corneal power estimated by IOL master and manual keratometry
Kumar P.1, Sreevathsala T.2, Tejaswini M.3, Konda K.4*
DOI: https://doi.org/10.17511/jooo.2021.i01.04
1 P. Sanjeeva Kumar, Associate Professor, Department of Ophthalmology, Santhiram Medical College and General Hospital, Kurnool, Andhra Pradesh, India.
2 T. Sreevathsala, Assistant Professor, Department of Ophthalmology, Santhiram Medical College and General Hospital, Kurnool, Andhra Pradesh, India.
3 M. Tejaswini, MBBS, Department of Ophthalmology, Santhiram Medical College and General Hospital, Kurnool, Andhra Pradesh, India.
4* Kavya Konda, Assistant Professor, Department of Ophthalmology, Santhiram Medical College and General Hospital, Kurnool, Andhra Pradesh, India.
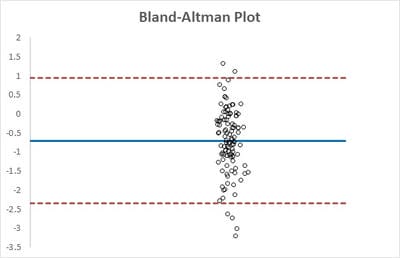
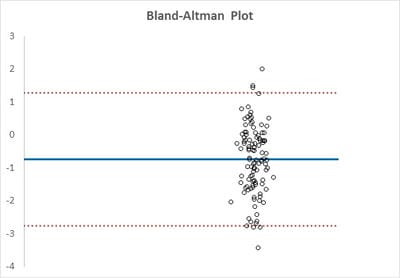
Aim: To compare corneal power calculated by IOL master and manual keratometry. Material & methods: A prospective, consecutive, comparative & single-centre study was done in pre cataract surgery work up patients. Manual keratometry was done using Keratometer KMS-6 (Appasamy Associates, India) while automated keratometry was done with IOL master 500 (Carl Zeiss Meditec, Jena, Germany). SPSS version 20.0 was used for statistical analysis. Results: Overall agreement between two methods was excellent for horizontal corneal diopteric power (kappa = 0.53 ) & good for vertical corneal diopteric power (kappa = 0.46) using bland-altman analysis. Conclusion: Manual keratometry is still relevant in the era of digital automated keratometry measured by IOL master.
Keywords: IOL master, keratometry, Corneal Power
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Ophthalmology, Santhiram Medical College and General Hospital, Kurnool, Andhra Pradesh, India. Email:  |
Kumar PS, Sreevathsala T, Tejaswini M, Konda K. Comparison of corneal power estimated by IOL master and manual keratometry. Trop J Ophthalmol Otolaryngol. 2021;6(1):18-21. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/180 |
 |
 ©
©