Swelling of the maxilla - A clinical enigma
Visakan Raja R.1, Gunasekara M.2*
DOI: https://doi.org/10.17511/jooo.2020.i05.03
1 Roopak Visakan Raja, Registrar, Department of Otorhinolaryngology and Head and Neck Surgery, Apollo Main Hospitals, Chennai, Tamil Nadu, India.
2* Manikandan Gunasekara, Assistant Professor, Department of Otorhinolaryngology, Shri Satya Sai Medical College and Research Institute, Chennai, Tamil Nadu, India.
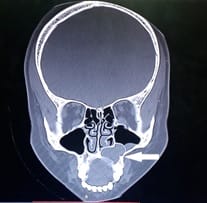
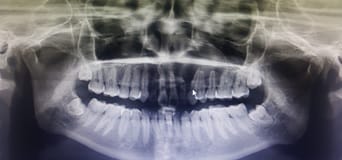
Swelling in the maxillary region, especially unilateral, is a surgical enigma. The condition is very rare but misleading as a variety of conditions can mimic it. A young female came to our outpatient department with swelling in the left nasolabial - maxillary region for the past 9 months. The swelling was firm with eggshell crackling sensation, tender, not resonant with normal skin. Clinical examination revealed mild elevation of the left nasal cavity floor with facial asymmetry. Intraorally, the swelling in the alveolus obliterated the gingivobuccal sulcus. CT showed evidence of a cystic lesion arising from the apices of the upper right medial incisor to the upper left first premolar. Oral and maxillofacial surgery opinion was sought, who claimed that there was an Ellis fracture of the upper left lateral incisor and also that the swelling was hard, extending up to the upper left second premolar. Orthopantomogram was ordered which revealed periapical radiolucency extending from right upper medial incisor to the second upper left premolar. This gave the impression of periapical pathology. Routine blood investigations were done and anesthetic fitness was obtained. The patient was taken up for cyst excision under general anesthesia. The cyst was enucleated completely and sent for histopathological examination. The pathology report came back as a dentigerous cyst. Thus a swelling in the maxillary region remains a diagnostic dilemma. Early diagnosis and appropriate radiological investigations are vital. Despite being uncommon in routine practice, it is vital for otolaryngologists to have adequate awareness, knowledge, and skills to deal with such conditions.
Keywords: Maxillary region, Surgical enigma, Swelling
| Corresponding Author | How to Cite this Article | To Browse |
|---|---|---|
| , Assistant Professor, Department of Otorhinolaryngology, Shri Satya Sai Medical College and Research Institute, Chennai, Tamil Nadu, India. Email:  |
Raja RV, Gunasekara M. Swelling of the maxilla - A clinical enigma. Trop J Ophthalmol Otolaryngol. 2020;5(5):112-115. Available From https://opthalmology.medresearch.in/index.php/jooo/article/view/146 |
 |
 ©
©